
COVID Jab deadlier than COVID for anyone under 80
All Global Research articles can be read in 51 languages by activating the “Translate Website” drop down menu on the top banner of our home page (Desktop version).
To receive Global Research’s Daily Newsletter (selected articles), click here.
Visit and follow us on Instagram at @globalresearch_crg and Twitter at @crglobalization.
***
Recent data analysis shows the COVID jab is deadlier than COVID-19 itself for anyone under the age of 80. For younger adults and children, there’s no benefit, only risk
All age groups under 50 years old are at greater risk of dying after receiving a COVID jab than an unvaccinated person is at risk of dying from COVID-19
For those under 18, the COVID jab increases their risk of dying from COVID-19. They’re also 51 times more likely to die from the jab than they are to die from COVID if not vaccinated
Only when you get into the 60 and older categories do the risks between the jab and COVID infection become about even. In the 60 to 69 age group, the shot will kill one person for every person it saves from dying of COVID, so it’s a tossup as to whether it might be worth it for any given person
Data suggest U.S. deaths reported to VAERS are underreported by a factor of 20
*
According to a cost-benefit analysis by Stephanie Seneff, Ph.D., and independent researcher Kathy Dopp, the COVID jab is deadlier than COVID-19 itself for anyone under the age of 80. The cost-benefit analysis1 looked at publicly available official data from the U.S. and U.K. for all age groups, and compared all-cause mortality to the risk of dying from COVID-19.
“All age groups under 50 years old are at greater risk of fatality after receiving a COVID-19 inoculation than an unvaccinated person is at risk of a COVID-19 death,” Seneff and Dopp conclude. For younger adults and children, there’s no benefit, only risk.
“This analysis is conservative,” the authors note, “because it ignores the fact that inoculation-induced adverse events such as thrombosis, myocarditis, Bell’s palsy, and other vaccine-induced injuries can lead to shortened life span.
When one takes into consideration the fact that there is approximately a 90% decrease in risk of COVID-19 death if early treatment is provided to all symptomatic high-risk persons, one can only conclude that mandates of COVID-19 inoculations are ill-advised.
Considering the emergence of antibody-resistant variants like Delta and Omicron, for most age groups COVID-19 vaccine inoculations result in higher death rates than COVID-19 does for the unvaccinated.”
Real-Life Risk Reduction Is Negligible
The analysis is also conservative in the sense that it only considers COVID jab fatalities that occur within one month of injection. Looking at the U.S. Vaccine Adverse Events Reporting System (VAERS), we’re now seeing that many of those who are dying got the jab around April 2021 or earlier, so we know the shots can significantly cut your life short even if they don’t kill you in the first month. As detailed in Seneff’s and Dopp’s paper:
“Absolute real-life risk reductions (ARRs) … from COVID inoculations vary from a low of negative 0.00007% (an increased risk of a COVID death from inoculation) for children under age 18 to a positive 0.183% (0.00183) risk reduction of a COVID death for persons over age 80 …
COVID vaccine inoculations increase risk of death and produce a net negative benefit, aka increased risk of death … for all age groups younger than 60 years old. In other words, the COVID inoculations cause a net increase, rather than decrease, in the likelihood of death for all persons under 60 years old.
For those over 60 years old, the benefit of COVID inoculations is negligible, ranging from a 0.0016% reduction in likelihood of death for a 60- to 69-year-old persons to a 0.125% reduction in likelihood of death for those over 80 years old. Because preventative treatments are often given to well persons, a vaccine is supposed to provide very small risk compared to benefit.
Thus, such high fatality risks (VFRs) versus low benefit of risk reduction (ARRs) from the COVID inoculations are not acceptable, especially considering that low-cost, effective treatments are available that would additionally reduce COVID-19 death rates by as much as 90% or more if provided as soon as symptoms appear in high-risk persons.”
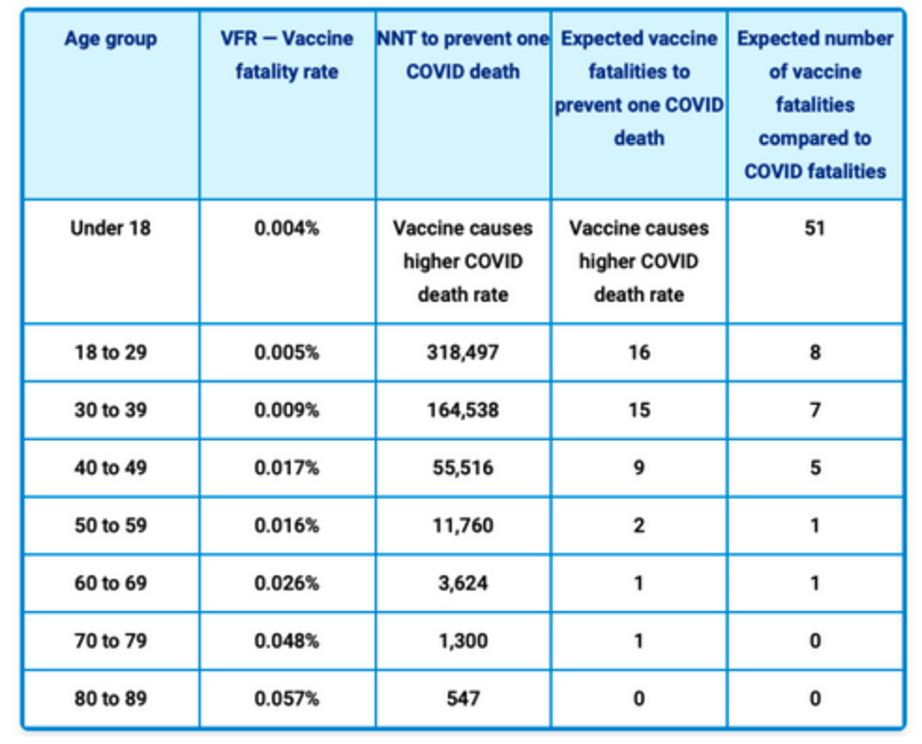
Meanwhile, data from an analysis2 by researchers Spiro Pantazatos and Herve Seligmann suggest U.S. deaths reported to VAERS are underreported by a factor of 20. Their analysis was used to calculate vaccine fatality rates (VFR), the number needed to treat/vaccinate (NNT) to prevent one COVID death, the expected number of vaccine fatalities to prevent one COVID death, and the expected number of vaccine fatalities compared to COVID fatalities by age group:3
Summary Findings
In summary, key findings in this paper include the following:
- For those under 18, the COVID jab increases their risk of dying from COVID-19; those under 18 are 51 times more likely to die from the jab than they are to die from COVID if not vaccinated.
- In those aged 18 to 29, the COVID jab is 16 times more likely to kill a person than save their life if they get COVID. They’re also eight times more likely to die from the jab than to die from COVID if not vaccinated.
- Those aged 30 to 39 are 15 times more likely to die from the COVID jab than prevent their death, and they’re seven times more likely to die from the inoculation than to die from COVID if not vaccinated.
- Those aged 40 to 49 are nine times more likely to die from the COVID jab than having it prevent their death, and they’re five times more likely to die from the jab than to die from COVID if not vaccinated.
- Those aged 50 to 59 are twice (2 times) more likely to die from the COVID inoculation than to prevent one COVID death, while their risk of dying from the jab or dying from COVID if unvaccinated is about the same.
Only when you get into the 60 and older categories do the risks between the jab and COVID infection even out. In the 60 to 69 age group, the shot will kill one person for every person it saves from dying of COVID, so it’s a tossup as to whether it might be worth it for any given person.
Cost-Benefit Analysis Must Drive Public Health Policy
Common sense tells us that COVID-19 vaccination policy ought to be rooted in a rational evaluation of the true costs and benefits, and to do that, we need to assess whether the jabs are beneficial or harmful, and to what extent. So far, governments have completely ignored the cost of this mass injection campaign, focusing solely on perceived or imagined (not proven) benefit.
Video: More Children Die from the COVID Shot Than from COVID
As a result, we’re looking at the worst public health disaster in known history. The greatest tragedy of all is that none of our public health officials has bothered to protect even the youngest among us.
As of February 11, 2022, there were 34,223 COVID jab injury reports in the U.S. involving children under the age of 17.
The OpenVAERS team recently started looking at injury reports in children aged 17 and younger, and to their shock, they found 34,223 U.S. reports involving this age group through February 11, 2022. You can find the Child’s Report here.4 This is a staggering number, considering the 12- to 17-year-olds have only been eligible for the shot since May 2021, and 5- to 11-year-olds since October 2021.5
Pfizer Withdraws EUA Application for Children Under 5
Interestingly, February 11, 2022, Pfizer abruptly withdrew its Emergency Use Authorization (EUA) application for children under 5.6,7 The question is why? According to the U.S. Food and Drug Administration and Pfizer, they want to collect more data on the effects of a third dose, as two doses did not produce expected immunity in 2- to 5-year-olds.8
Three days later, former FDA Commissioner and current Pfizer board member Dr. Scott Gottlieb told CNBC9 the EUA application was pulled because COVID cases are so low among young children that the shot couldn’t be shown to provide much of a benefit.
But according in an email notice to subscribers, OpenVAERS stated, “None of these explanations suffice because all of that information was known prior to Pfizer submitting this EUA to the FDA on February 1 [2022]. It makes one wonder whether adverse events in the treatment group might be the factor that neither Pfizer nor the FDA want to talk about?”
Those Who Should Be in the Know Don’t Know a Thing
In related news, Jessica Rose, Ph.D., a research fellow at the Institute for Pure and Applied Knowledge in Israel, highlighted a February 5, 2022, Freedom of Information Request sent to the Therapeutic Goods Administration (TGA), the Australian equivalent of the FDA.10 The inquiry asked for documents relating to the TGA’s assessment of:
- The presence and risk of micro-RNA sequences within the Comirnaty mRNA active ingredient (the mRNA genomic sequence)
- The presence and risk of oncomirs (cancer-causing micro-RNA) in Comirnaty
- The presence and risk of stop codon read-through (suppression of codon activity) arising as a result of the use of pseudouridine in Comirnaty
- The composition of the final protein product (molecular weight and amino acid sequence) produced following injection of the Comirnaty mRNA product in human subjects
- The risk of the use of AES-mtRNR1 3’ untranslated region of the Comirnaty mRNA product in human subjects
As it turns out, the TGA has none of these documents, because they’ve not assessed any of these risks. Why does this matter? Well, as explained by Rose:
“Micro-RNA (miRNAs) are small (20-22 nucleotides) single-stranded non-coding RNA molecules that function to interrupt or suppress gene expression at transcriptional or translational levels to regulate gene expression.”
Considering micro-RNA can alter gene expression, wouldn’t we want to know if micro-RNAs are present in the shot, considering we’re injecting hundreds of millions of people, including teenagers and children? The same goes for oncomirs, the suppression of codon activity, protein products and the rest.
“Stephanie Seneff has warned11 of two miRNAs that disrupt the type-1 interferon response in any cell, including immune cells: miR-148a and miR-590,” Rose continues.
“I don’t know what potential connections there are here yet, but it is safe to say that any tech that involves the introduction of foreign mRNA to be mass-produced by human cells must be thoroughly safety tested.
The fact that none of these documents ‘exist’ is proof positive that they either have no idea what the potential effects of what they made are because they did no bench work/investigations/studies, or, that they know and are hiding the results. Either choice is beyond criminal.”
The Critical Design Flaw
In an August 2021 Substack article,12 British cybersecurity researcher Ehden Biber homed in on the potential risks of using pseudouridine to optimize the codon.
The COVID shots do not contain the identical mRNA found in the SARS-CoV-2 virus. The mRNA has been genetically manipulated in a process called “codon optimization,” and this process is actually known to create unexpected and detrimental side effects.
“How come Pfizer, Moderna, AstraZeneca, Janssen etc. are using a technology that both they and the regulators know will cause unknown results?” Biber asked. The reason codon optimization was used is because it’s pretty difficult to get your body to produce a given protein by injecting mRNA.
It’s a slow and generally inefficient process. In order for the injection to work, they need higher levels of protein expression than is naturally possible. Scientists bypass this problem by making substitutions in the genetic instructions. They’ve discovered that you can swap out certain nucleotides (three nucleotides make up a codon) and still end up with the same protein in the end. But the increased efficiency comes at a terrible cost.
When substituting parts of the code in this way, the resulting protein can easily get misfolded, and this has been linked to a variety of chronic diseases,13 including Alzheimer’s, Parkinson’s disease and heart failure.14 As explained by Biber:15
“Turns out the protein which was manufactured when codon optimization has different ways it folds and a different 3D shape, and it ‘could cause immunogenicity, for example, which wouldn’t be seen until late-stage clinical trials or even after approval.’ This statement relates to the NORMAL approval cycle. The COVID vaccines went via an accelerated one.”
Now, the FDA has been fully aware of these problems since 2011, when Chava Kimchi Sarfaty, Ph.D., a principal investigator at the FDA, stated that “We do not believe that you can optimize codons and have the protein behave as it did in its native form.”
She went on to warn, “The changed form could cause immunogenicity, for example, which wouldn’t be seen until late-stage clinical trials or even after approval.”16
If the FDA knew all this back in 2011, why have they not raised objections against codon optimization being used in the making of the COVID jabs? The same question needs to be asked of the Australian TGA.
The FOIA requester was likely thinking of the March 2021 paper, “BNT162b2 Vaccine: Possible Codons Misreading, Errors in Protein Synthesis and Alternative Splicing Anomalies”17 when they put together that inquiry, because that paper highlights Pfizer’s extensive codon optimization using pseudouridine, which has known adverse effects, as well as the use of 3’-UTR sequence, the consequences of which are still unknown.
The fact that the TGA has no data on the risks of these modifications just goes to show that they, like the U.S. FDA, are not actually working to ensure these jabs are safe. They’re protecting the profits of the drug companies.
Pfizer even admits, in its BNT162b2/Comirnaty Risk Management Plan submitted to the FDA to get EUA, that the codon optimization they did resulted in elevated gamma-glutamyl transferase (GGT),18which is an early marker of heart failure. Elevated GGT is also an indicator of insulin resistance, cardiometabolic disease,19 liver disease20 and chronic kidney disease.21
That alone should have raised some questions, were the FDA actually looking out for public health. All in all, there’s more reason than ever to question the COVID jab mandates and the use of these shots in children.
*
Note to readers: Please click the share buttons above or below. Follow us on Instagram, @globalresearch_crg. Forward this article to your email lists. Crosspost on your blog site, internet forums, etc.
Notes
1 COVID-19 and All-Cause Mortality Data Analysis by Kathy Dopp and Stephanie Seneff (PDF)
2 COVID Vaccination and Age-Stratified All-Cause Mortality Risk (PDF)
5 Yale Medicine October 25, 2021, Updated February 11, 2022
6 New York Times February 12, 2022
10 Jessica Rose Substack February 20, 2022
11 Extremely American August 1, 2021
12, 15, 16 Ehden Substack August 20, 2021
13 Nature Medicine December 6, 2011; 17: 1536-1538
14 Autophagy August 2008; 4(6): 821-823
17 Authorea March 25, 2021 DOI: 10.22541/au.161668243.35142344/v1
19 European Journal of Preventive Cardiology 2014 Dec;21(12):1541-8
20 Disease Markers October 12, 2015; 2015: 818570
21 Disease Markers 2017; 2017:9765259
Featured image is from The Liberty Daily
The original source of this article is Mercola
Copyright © Dr. Joseph Mercola, Mercola, 2022